This blog post reports on work-in-progress within the DfG course! The post is written by group 2B dealing with the Kela and the Ministry of Social Affairs and Health’s brief on Continuity of Care as a new Kela reimbursement model. The group includes Bhairavi Balasubramanian and Sofia Correia from the Masters Programme in Collaborative Industrial Design, and, David Bertl and Tuomas Laakkonen Masters Programme in Creative Sustainability
Written by: Tuomas Laakkonen
Medical emergency
I am a Finnish citizen, but I grew up in Norway, and consequently I grew up with fantastic healthcare and a personal doctor in the public sector. When I moved to Finland 4 years ago and started working, I was confused that I would need some kind of healthcare coverage from my work. This confusion continued when I started studying and received the first notice of korkeakouluopiskelijan terveydenhoitomaksu, words I had to read 5 times before realizing what they meant. For non-Finnish people (and possibly some Finns), the healthcare system here is highly perplexing, In the past weeks my teammates and I have been unravelling its structural mysteries and plotting a strategy for applying change to pressing systems level challenges.
Bowtie of possibilities
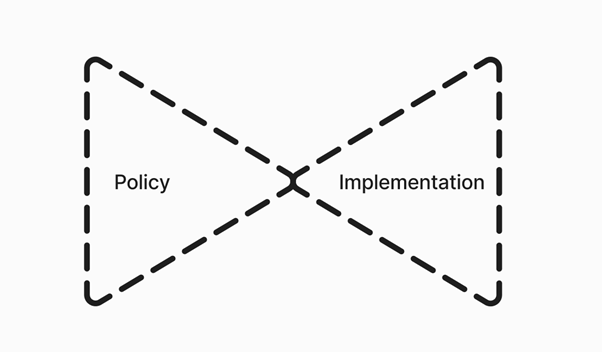
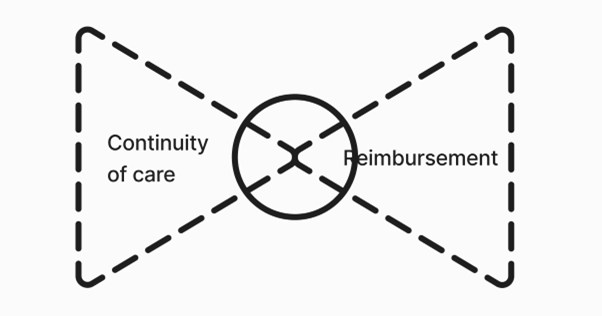
Government Bowtie © Creative Commons CC by 4.0 2024. Bhairavi Balasubramanian, Sofia Correia, David Bertl and Tuomas Laakkonen. Design for Government. Aalto University.
The above bowtie illustrates the process of policy development and implementation. This figure illustrated what I think might be the biggest difference between designing for parts of government and other design projects. As designer I am used to following the double diamond, a framework where the designer woks in a more linear path of research and implementation (The Double Diamond – Design Council, n.d.). In contrast, my bowtie describes a more circular approach, here the knot in this tie is the designer, who facilitates the information flow between policy and implementation.
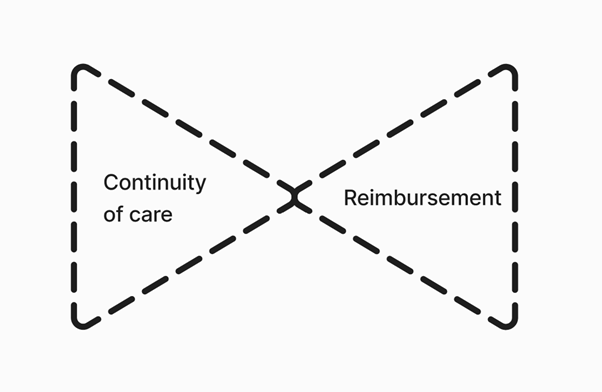
Brief Bowtie © Creative Commons CC by 4.0 2024. Bhairavi Balasubramanian, Sofia Correia, David Bertl and Tuomas Laakkonen. Design for Government. Aalto University.
At first glance our team felt that it was difficult to understand the connection between Kela’s planned reimbursement model, and the overall goal of improving continuity of care. I think this was simply our double diamond eyes looking at a bowtie problem. It is more helpful to think of continuity of care as the policy and reimbursement model as first step of implementation. Our task will be to understand how this first step can be taken to create momentum towards continuity of care. To build this momentum, we must first understand the deeper challenges of the system.
Knock knock… Who’s there?

Doors to Healthcare © Creative Commons CC by 4.0 2024. Bhairavi Balasubramanian, Sofia Correia, David Bertl and Tuomas Laakkonen. Design for Government. Aalto University.
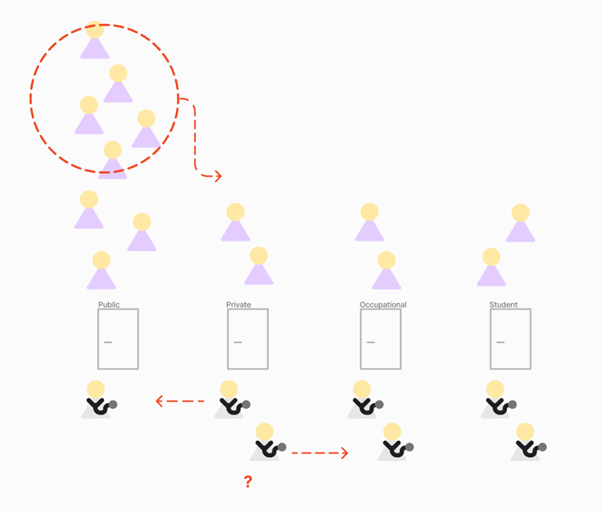
Simplifying the healthcare system a bit, we can consider that access to the Finnish healthcare system primarily happens through one of four doors. These doors are ways to access the general practitioners that can possibly refer patients further into specialized healthcare. The doors are divided into Public-, Private-, Occupational- and Student Healthcare. In reality, the doors are a bit more intertwined, with complex hallways and secret passages. For now, however, we can limit ourselves to think of them as simple cedarwood doors. Enabling equal access to all users of healthcare services is a key issue that must be solved to increase continuity of care. In practice, this means that the lines to the doors and the number of doctors turning the handle needs to be equal across services. Currently, the situation is rather different; the door to public healthcare has a long line of patients waiting, and relatively few doctors letting people in. In contrast, private services have more doctors, and the door is wide open for the few patients coming through. So where do we go from here?
Doors to Healthcare 2 © Creative Commons CC by 4.0 2024. Bhairavi Balasubramanian, Sofia Correia, David Bertl and Tuomas Laakkonen. Design for Government. Aalto University.
First steps towards continuity of care are already planned and seek to equalize the lines of patients by enabling users of the public doors to knock on private ones. Kela is planning to do this through patient reimbursements, while the Western Uusimaa Wellbeing Services County will be running a trial where Doctors working as entrepreneurs can receive patients from the public sector. These models assume that general practitioners prefer working in the private sector because of the current working conditions and level of autonomy. Based on our roundtable discussion, our team is not convinced that these efforts will render all doors equal, or if it will just shift the problems from one part of the system to another.
Doors to Healthcare Motivations © Creative Commons CC by 4.0 2024. Bhairavi Balasubramanian, Sofia Correia, David Bertl and Tuomas Laakkonen. Design for Government. Aalto University.
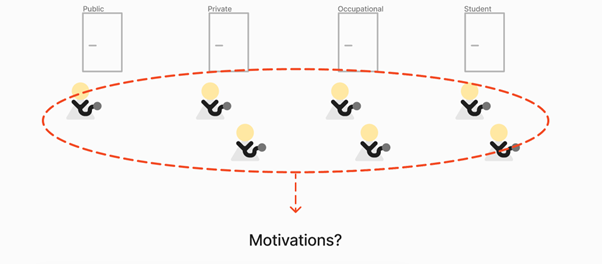
“But how can financial incentives impact working conditions?”
In our group we have decided to focus on the needs of the general practitioners across the four doors. Through understanding their needs, motivations, and working we hope to understand how we could possibly maintain the existing number of general practitioners and recruit new ones. In addition, we hope to expand the understanding of the general practitioners to include the nurses and supporting staff to understand ways to make the doctors time as meaningful as possible. Understanding these fundamentals is key in the work towards increased continuity of care in the long perspective. But how can financial incentives impact working conditions?
It’s all about leverage
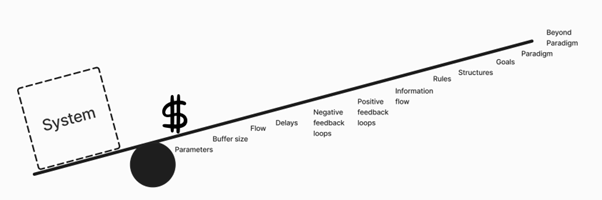
Leverage (Based on Meadows, 2009) © Creative Commons CC by 4.0 2024. Bhairavi Balasubramanian, Sofia Correia, David Bertl and Tuomas Laakkonen. Design for Government. Aalto University.
“As a first step this would be a giant leap…”
With the new reimbursement model Kela is trying to achieve deeper impact in the healthcare system, and in the long run increase continuity of care. This is a difficult task, because money is not a strong point of leverage for systems changes, at least according to my favourite scholar; Donella Meadows. According to Meadows there are 12 possible points of leverage in a system (2009) And although politicians and larger society often argue about taxation and funding of different ventures, money is considered to have little overall effect in systems change. So, taxation is theft and politics useless? Well, the flow of money can have larger impact on a system, when it flows in a way that reaches deeper leverage points. We have hypothesized that by researching the working conditions of doctors in primary healthcare, we might find deeper leverage points that can be indirectly targeted by Kela reimbursements. As a first step this would be a giant leap towards continuity of care. In addition, we would need to develop a method for measuring the success of this new model. if we can do that, we will reinforce the communication between implementation and policy, and the initial leap might developed into a full sprint.
Leverage (Based on Meadows, 2009) © Creative Commons CC by 4.0 2024. Bhairavi Balasubramanian, Sofia Correia, David Bertl and Tuomas Laakkonen. Design for Government. Aalto University.
Future appointments
Despite the grand vision of outcomes, it is important to remind ourselves that we are only in the beginning of this journey, and truth be told, continuity of care is an eternity project. For now, we have only gotten a first glance at an infinitely complex system. Yet we have found that understanding the general practitioners’ needs, motivations, and working conditions across the healthcare systems is key to developing applicable changes to the industry that can shift the system towards increased continuity of care for all patients. I hope that at the end of this project we will be able to provide data that will inform policy making and implementation towards increased continuity of care.
Sources:
Meadows, D. (2009). Thinking in systems : a primer (Diana. Wright, Ed.) [Book]. Earthscan.
The Double Diamond – Design Council. (n.d.). Retrieved March 19, 2024, from https://www.designcouncil.org.uk/our-resources/the-double-diamond/
The DfG course runs for 14 weeks each spring – the 2024 course has now started and runs from 26 Feb to 29 May. It’s an advanced studio course in which students work in multidisciplinary teams to address project briefs commissioned by governmental ministries in Finland. The course proceeds through the spring as a series of teaching modules in which various research and design methods are applied to address the project briefs. Blog posts are written by student groups, in which they share news, experiences and insights from within the course activities and their project development. More information here about the DfG 2024 project briefs. Hold the date for the public finale on Wednesday 29 May!