This blog post reports on work-in-progress within the DfG course! The post is written by group 2A dealing with Kela and the Ministry of Social Affairs and Health’s brief on continuity of care. The group includes Emma Prost and Atte Kuparinen from the Collaborative and Industrial Design program, and Beste Polatkal and Thekla Weißkopf from the Creative Sustainability Design program.
Written by: Emma Prost
Recap.
Since our last update, our group 2A has been analysing the administrative challenges faced by Finland’s public healthcare system. Through interviews, research, and workshops, we’ve identified excessive administrative burdens on doctors and nurses as a primary obstacle to providing continuous, high-quality patient care (General Practitioner, nurses and medical secretary, May 10, 2024; General Practitioner, personal communication, March 2024). Our interviews revealed that non-medical tasks such as paperwork and cleaning are significantly reducing the time healthcare professionals can dedicate to patient care. Additionally, workshops highlighted the detrimental impact of these tasks on job satisfaction and stress levels among medical staff. This insight has shaped our design proposal, which aims to alleviate these burdens and enhance the efficiency of the healthcare team.
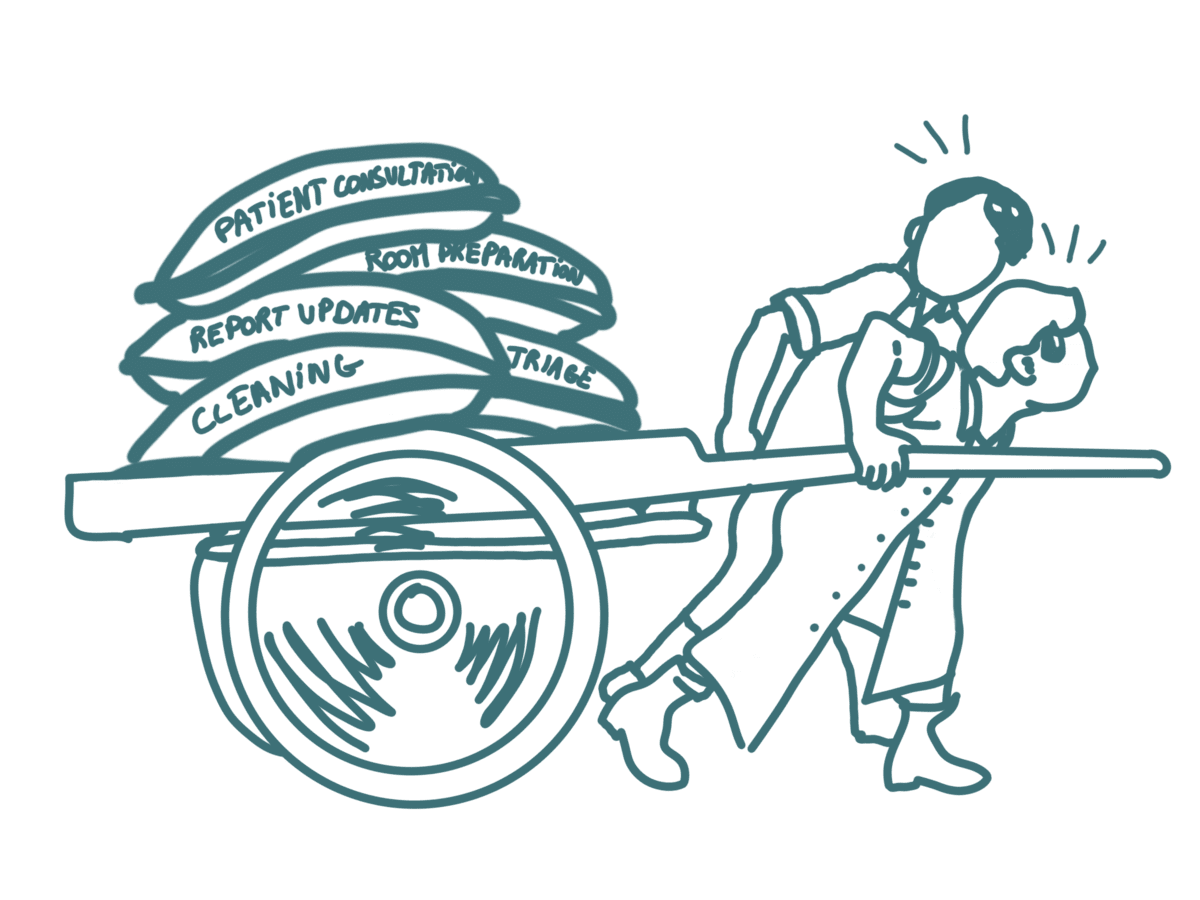
Our research revealed that doctors and nurses are oppressed by non-medical tasks, such as paperwork and cleaning, which significantly reduce their time for patient care. For example, nurses now clean the common fridge, and doctors clean their desks and refill their printers—tasks that could be done by someone without a medical degree, saving time for both doctors and nurses. This administrative overload not only increases stress and job dissatisfaction but also drives medical professionals to leave the public sector or reduce their working hours. If this trend continues, Finland’s public healthcare system faces a potential shortage of general practitioners (GPs), which will severely impact the continuity of patient care (Yle News, 2021; General practitioner, nurses and medical secretary, May 10, 2024).
 VS
VS
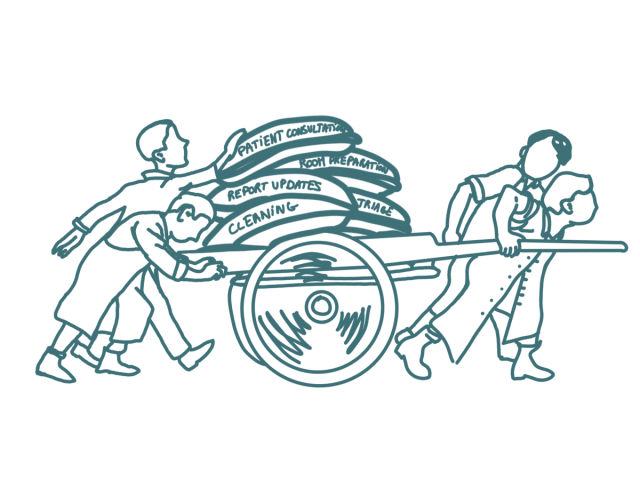
Two different team structures compared for a same workload. © CREATIVE COMMONS CC BY 4.0 2024 ATTE KUPARINEN, BESTE POLATKAL, EMMA PROST AND THEKLA WEISSKOPF DESIGN FOR GOVERNMENT COURSE AT AALTO UNIVERSITY
A (new?) Entry Point to Continuity of Care
So, our goal is clear: we must alleviate the pressure on these medical team members to prevent them from feeling compelled to leave the public sector. Our entry point proposal involves rethinking the distribution of tasks within the medical team responsible for continuous patient care. By ensuring that doctors and nurses focus on medical tasks they are trained for and passionate about, we can enhance efficiency and job satisfaction. This approach will help prevent leakage to the private sector or part-time work and avert the future threat of a doctor’s shortage. Redistributing tasks could also involve welcoming another team member, such as a medical assistant, to handle cleaning and paperwork that doctors and nurses currently manage.
Surprisingly, we learned that redistributing tasks and including medical assistants was implemented in the past (Kokko, 2009; General practitioner, nurses and medical secretary, May 10, 2024). The medical team previously included medical assistants who managed administrative and non-medical tasks, allowing doctors and nurses to focus on patient care, diagnosis, and treatment. However, these medical assistants were laid off due to budget cuts, not because they were unnecessary. In fact, several doctors and nurses we interviewed said they miss these assistants today (General practitioner, nurses and medical secretary, May 10, 2024). Thus, our idea of redistributing tasks still holds.
The Strategic Shift: Presenting a Cost-Effective Proposal
However, this unexpected learning of a medical assistant in past medical team introduced a big shift in our approach to Kela and the Ministry of Social Affairs and Health. Indeed, since medical assistants were previously part of the team, we need to present a compelling argument for their reintroduction. Instead of merely showing that medical assistants are needed for the continuity of care –which they probably know already since they tried this idea before, we must convince our partners that it is not only necessary but also cost-efficient. We must speak their language.
A Necessary Delay in Our Reach for Continuity of Care
Throughout this project, we were tasked with ensuring continuity of care, comparable to guiding a cart (patient care) to its destination (continuity of care). However, the “horses” (medical team) pulling the cart are overburdened and exhausted, having to fill in for the medical assistants who were let go. To prevent the horses from dropping out due to exhaustion or dissatisfaction, we need to prepare them adequately.
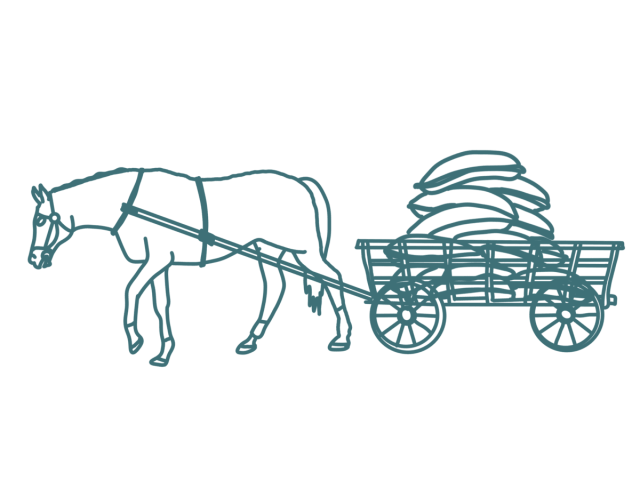 VS
VS
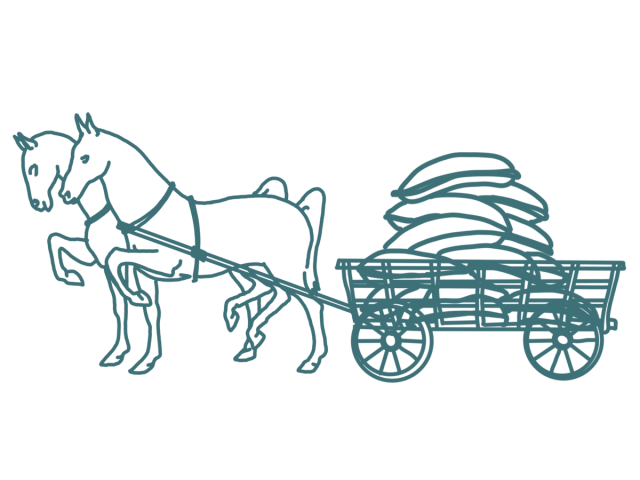
One horse versus two horses dragging a same weight. © CREATIVE COMMONS CC BY 4.0 2024 ATTE KUPARINEN, BESTE POLATKAL, EMMA PROST AND THEKLA WEISSKOPF DESIGN FOR GOVERNMENT COURSE AT AALTO UNIVERSITY
By reinstating a well-balanced division of tasks among medical team members, each task necessary for providing quality and continuous patient care would be handled by trained professionals. Likewise, if more horses are added to the cart, they will be more efficient together, and the cart could advance in the right direction. So, horses first, cart and its direction later. Medical team first, continuity of care later. Prioritization is crucial. First, we must repair the broken team structure; then, we can work on making healthcare cost-effective and oriented towards continuity of care.
The reintroduction of medical assistants is vital for reducing the administrative burden on doctors and nurses, which in turn enhances job satisfaction and improves patient care quality. By restructuring the healthcare team and ensuring each member operates within their area of expertise, we can address the imminent shortage of GPs and secure a sustainable future for Finland’s public healthcare system. Stay tuned for our upcoming proposal video and report, where we will share detailed planning and collaboration with stakeholders to implement these changes effectively!
References
- Workshop with anonymous healthcare professionals (May 10, 2024).
- General Practitioner. (March 2024). Personal interview. [Anonymous].
- Yle News. (2021, August 22). Finland faces public sector doctor shortage. Yle. https://yle.fi/a/3-12068233
- Kokko S. Integrated primary health care: Finnish solutions and experiences. Int J Integr Care. 2009 Jun 25;9:e86. doi: 10.5334/ijic.310. PMID: 19590612; PMCID: PMC2707593.
The DfG course runs for 14 weeks each spring – the 2024 course has now started and runs from 26 Feb to 29 May. It’s an advanced studio course in which students work in multidisciplinary teams to address project briefs commissioned by governmental ministries in Finland. The course proceeds through the spring as a series of teaching modules in which various research and design methods are applied to address the project briefs. Blog posts are written by student groups, in which they share news, experiences and insights from within the course activities and their project development. More information here about the DfG 2024 project briefs.